Не все знают, что МРТ коленного сустава дает не стопроцентный результат диагностики, так как интерпретация снимков МРТ требует определенного опыта, который есть не у всех врачей. В результате неправильной расшифровки МРТ-картины диагноз может быть поставлен неточно или неверно. Ниже представлены распространенные диагностические ошибки при МРТ коленного сустава.
Частые ошибки МРТ коленного сустава
Степень разрыва мениска по Столлеру (Stoller) может быть выставлена неверно, что влечет за собой ненужную операцию или неправильное лечение. Помните, что не все повреждения мениска требуют операции!
Неправильный диагноз разрыв мениска. По МРТ может быть диагностирован разрыв мениска, в то время как на самом деле мениск нормальный. Существуют нормальные варианты строения мениска, которые неопытный врач может принять за повреждение. В результате назначается ненужная артроскопическая операция на колене. Недобросовестные врачи-травматологи тоже склонны трактовать спорные изменения в пользу разрыва, ведь тогда они смогут заработать на дорогой операции.
Псевдоразрыв мениска на МРТ. При первичном анализе МРТ диагностирован разрыв. На самом деле имеется нормальный вариант строения, обусловленный менискофеморальной связкой Рисберга.
Импрессионный перелом на МРТ нередко просматривается врачами. Причина — слабое знакомство с рентгенологической картиной небольших импрессионных переломов мыщелков.
Длительные боли в колене довольно часто ошибочно связываются с травмой, тогда как настоящая их причина — это воспалительные заболевания, например ревматоидный артрит, подагра и другие артропатии. Ревматоидный артрит на МРТ имеет характерные признаки, на которые часто не обращают внимания.
Разрыв передней или задней крестообразной связки может быть диагностирован неправильно: вместо полного разрыва указан частичный, вместо хронической мукоидной дегенерации – острый отек, и т.п. Иногда пропускается разрыв связки.
Болезнь Гоффа на МРТ. Рентгенолог может забыть оценить состояние жирового тела надколенника, при том что болезнь Гоффа — это не очень приятное заболевание, приносящее много страданий.
Редкие болезни коленного сустава могут с трудом диагностироваться на МРТ. Врач может не увидеть или неправильно трактовать виллонодулярный синовит, синдром медиопателлярной складки, синдром илиотибиального тракта, разрыв заднелатерального комплекса и другие редкие болезни.

Первый диагноз — перелом надколенника (коленной чашечки). На самом деле здесь нормальный вариант развития — patella bipartita (надколенник состоит из двух частей).
Как избежать ошибок в чтении мрт коленного сустава?
Чтобы избежать ошибок МРТ, после его прохождения всегда лучше показать результаты специалисту, который предметно занимается диагностикой болезней костей и суставов. Лучше всего обратиться к рентгенологу, имеющему большой опыт в костно-суставной патологии. Такие специалисты представлены в Национальной телерадиологической сети. Эта служба консультаций врачей-радиологов объединяет специалистов из крупных профильных центров, и ее услугами пользуются клиники и пациенты из многих городов России. Вы можете отправить результаты МРТ для пересмотра с помощью специального сервиса, и получить уже через 24 часа подробное заключение рентгенолога с подписью.

Кандидат медицинских наук, член Европейского общества радиологов
- Расценки
- Главная
- Акции
- Запись на МРТ
- Контакты
- Обо мне
- Обратная связь
- Безопасность МРТ
- Отзывы
- Популярно об МРТ
![]()
- Расценки
- Главная
- Акции
- Запись на МРТ
- Контакты
- Обо мне
- Обратная связь
- Безопасность МРТ
- Отзывы
- Популярно об МРТ
Магнитно-резонансная томография (МРТ) в Санкт-Петербурге
![]() (812) 493-39-22
(812) 493-39-22

Запишитесь на МРТ по телефону
(812) 493-39-22
или заполните форму

Расписание приема МРТ:
ЦМРТ Нарвская
(812) 493-39-22
Среда и воскресенье: с 08:00 до 23:00
ул. Ивана Черных, 29
МРТ аппарат 1,0 Тл
ЦМРТ Старая Деревня
ул. Дибуновская, 45
Четверг, суббота: с 08:00 до 23:00
МРТ аппарат 1,5 Тл
- Как выбрать место МРТ
- Головной мозг
- МРТ турецкого седла
- МР-ангиография (сосудистая программа)
- МРТ энциклопедия головного мозга
- Позвоночник
- МРТ шейного отдела позвоночника
- МРТ поясничного-крестцового отдела позвоночника
- МРТ энциклопедия позвоночника
- Брюшная полость
- МР-холангиография
- МРТ-энтерография (гидро-МРТ)
- Суставы
- Коленный сустав
- МРТ энциклопедия коленного сустава
- Малый таз
- Надпочечники
- Почки
- МРТ мягких тканей
- МРТ-маммография
- МРТ на аппаратах открытого типа
- МРТ для остеопатов
- Основы лучевой диагностики для студентов-медиков
Типичные ошибки при МРТ коленного сустава
МРТ коленного сустава отличается высочайшей чувствительностью при травмах и других патологиях. Вместе с тем, встречаются необычные варианты строения сустава, принимаемые при МРТ за патологию. При МРТ в СПб мы в наших клиниках всегда внимательно оцениваем анатомические варианты, чтобы не принять их при МРТ коленного сустава за травматические повреждения.
Место прикрепления менискофеморальной (Ризберга) связки к заднему рогу латерального мениска при МРТ коленного сустава иногда принимают за косой разрыв мениска. Связка Ризберга прикрепляется позади задней крестообразной связки, примерно на 14 мм латеральнее ее. Если высокий сигнал при МРТ коленного сустава виден дальше этого места, то разрыв вполне возможен. Однако надо еще учитывать, что менискофеморальная связка обычно разрывается вместе с передней крестообразной связкой.

МРТ коленного сустава. Т2-взвешенная сагиттальная МРТ. Связка Ризберга симулирующая при МРТ разрыв заднего рога латерального мениска.
Пересечение заднего рога латерального мениска сухожилием подколенной мышцы также может симулировать на МРТ коленного сустава в сагиттальной плоскости горизонтальный разрыв.

МРТ коленного сустава. Сагиттальная Т2-взвешенная МРТ. Псевдоразрыв мениска – сухожилие подколенной мышцы.
Со стороны медиального мениска при МРТ коленного сустава в сагиттальной плоскости изредка встречаются менискокапсульные карманы, очень напоминающие менискокапсульные разрывы.

МРТ коленного сустава. Т2-взвешенная сагиттальная МРТ. Менискокапсульный карман.
Дисковидные мениски, наблюдаемые с латеральной стороны, тоже могут симулировать смещение диска. То же может быть и при выраженной мениско-менисковой связке, “наползающей” при МРТ коленного сустава в межмыщелковую вырезку.

МРТ коленного сустава. Т2-взвешенная сагиттальная МРТ. Косая мениско-менисковая связка.
Остались вопросы? Звоните +7 (812) 493-39-22 или оставьте свои данные и мы
Вам перезвоним!
- Research
- Open Access
- Published: 02 June 2008
- Efstathios Chronopoulos2,
- Christianna Savvidou2,
- Spyros Plessas2,
- Peter Giannoudis1,
- Nicolas Efstathopoulos2 &
- …
- Georgios Papachristou2
Journal of Trauma Management & Outcomes
volume 2, Article number: 4 (2008)
Cite this article
-
17k Accesses
-
45 Citations
-
11 Altmetric
-
Metrics details
Abstract
Background
Many surgeons tend to believe that MRI is an accurate, non invasive diagnostic method, enough to lead to decisions for conservative treatment and save a patient from unnecessary arthroscopy. We conducted a retrospective study to investigate the accuracy of the MRI of the knee for the detection of injuries of the meniscus, cruciate ligaments and articular cartilage, in comparison with the preoperative clinical examination and intraoperative findings. Between May 2005 and February 2006 102 patients after clinical examination were diagnosed with meniscal or cruciate injury and underwent definitive treatment with arthroscopy. 46 of these patients fulfilled the inclusion criteria. The accuracy, sensitivity, specificity, negative and positive predictive values of the MRI findings were correlated with the lesions identified during arthroscopy. The diagnostic performance of the initial clinical examination was also calculated for the meniscal and cruciate ligament injuries.
Results
The accuracy for tears of the medial, lateral meniscus, anterior and posterior cruciate ligaments and articular cartilage was 81%, 77%, 86%, 98% and 60% respectively. The specificity was 69%, 88%, 89%, 98% and 73% respectively. The positive predictive value was 83%, 81%, 90%, 75% and 53% respectively. Finally, the clinical examination had significant lower reliability in the detection of these injuries.
Conclusion
MRI is very helpful in diagnosing meniscal and cruciate ligament injuries. But in a countable percentage reports with false results and in chondral defects its importance is still vague. The arthroscopy still remains the gold standard for definitive diagnosis.
Peer Review reports
Background
Arthroscopy is considered as «the gold standard» for diagnosis of traumatic intraarticular knee lesions [1]. However, arthroscopy is an invasive procedure that requires hospitalization and anaesthesia, thus presenting all the potential complications of a surgical procedure [2]. Since it’s introduction in the 1980’s Magnetic Resonance Imaging (MRI) has gained in popularity as a diagnostic tool of the musculoskeletal disorders [3]. Especially the knee is the most frequent examined joint with MRI. Many surgeons tend to believe that MRI is an accurate, non invasive diagnostic method of the knee injuries, enough to lead to decisions for conservative treatment and save a patient from unnecessary arthroscopy. Nevertheless, even nowadays, remains very expensive. Taking in account that health-economics play important role in patients management, many questions arise regarding when and how often one must ask for an MRI when clinical examination has already confirm the diagnosis of meniscal tear or cruciate ligament rupture [4]. The opposite question might be more important; is negative MRI enough to prevent unnecessary arthroscopy, when clinical examination suggests a meniscal or cruciate ligament injury?
With the purpose of investigating the accuracy of magnetic resonance imaging in patients with clinical signs of traumatic intraarticular knee lesions, we compared its findings with those obtained from the subsequent arthroscopies.
Methods
After obtaining the approval of the hospital ethics committee, we retrospectively reviewed the case notes of patients who had been clinically diagnosed with meniscal or cruciate injury, between May 2005 and February 2006 in our institution. Patients who had subsequently undergone further examination with MRI and were definitively treated with arthroscopy were then identified. We adhered to the Standards for Reporting of Diagnostic Accuracy (STARD) criteria for design and presentation of diagnostic studies [5]
Patients that in plain X-rays had fractures, loose bodies or signs of severe osteoarthritis were excluded from the study. Additionally, patients that after the MRI examination have had new injury to the same knee, before the arthroscopy or delayed to undergo arthroscopy for more than 3 months, were also excluded.
All patients had thorough clinical examination from two experienced knee surgeons prior to the MRI. Clinical examination focused on meniscal injury and cruciate ligament injury. The tests used in the clinical diagnosis were: the anterior-posterior drawer test, the Lachman test, the pivot shift test for the diagnosis of cruciate ligament injuries and the Apley’s and McMurray’s test for the meniscal injuries [6].
MRI examinations were performed in 2 different diagnostic centres. The MRI scanners were two 1.5 tesla units (Philips Medical Systems). T1 and T2 weighted images in coronal, axial and sagittal planes were obtained. Slice thickness ranged from 3 to 5 mm. The films were interpreted from 2 experienced knee radiologists who were aware of the result of the clinical examination as this was written at the initial referral letter. Any abnormalities of the cruciate ligaments, menisci or hyaline cartilage were described on a standard form. Preoperatively each MRI was also assessed by the surgeon performing the arthroscopy. In the case of different opinions between the two, the radiologists’ diagnosis was considered more reliable.
All arthroscopies were performed by 2 experienced knee surgeons in a hospital environment with complete preoperative and postoperative care. A 4 mm Karl-Storz arthroscope with a 30-degree angle was used. Standard arthroscopic portals were used. ; the inferolateral portal for the arthroscope, and the inferomedial portal for the probe. Before any intervention, all knee interior structures were examined with the probe. Chondral defects were classified as positive if were more than 2nd grade according to the Outerbridge classification [7] and measured more than 1 cm in diameter. A cruciate ligament was considered to be torn if it was completely disrupted at one of its attachments to bone or in its substance, or if laxity (partial tear) could be demonstrated with a probe. All arthroscopic findings were photographed and registered. For further evaluation all arthroscopic findings were considered accurate and served as reference base.
MRI diagnoses and clinical findings were placed into one of four categories after arthroscopic evaluation. A result was considered a true-positive if the clinical or MRI diagnosis was confirmed by arthroscopic evaluation. A result was considered a true-negative if the diagnosis of no tears was confirmed by arthroscopy. A result was considered a false-positive if the arthroscopy was negative but the results were positive at the clinical examination or on the MRI. If the arthroscopy was positive but the clinical examination and MRI were negative, this was considered a false-negative result.
Statistical analysis was used to calculate sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV), in order to assess the realibility of the clinical and MRI results. 95% confidence intervals for sensitivity and specificity, as well as positive (LR+) and negative likelihood ratios (LR-) and areas under the ROC curve (AUC) were calculated.
Results
One hundred two patients after clinical examination were diagnosed with meniscal or cruciate injury and underwent definitive treatment with arthroscopy, during the studied period. After the application of the exclusion criteria we were able to identify 46 patients (30 males) that were further examined with MRI preoperatively. The mean age was 32 (18 – 45) years. Right knee injury presented to 21 whereas left knee injury to 25 patients. Table 1 summarizes the patients’ demographics. Arthroscopy revealed 33 medial meniscus tears, 21 lateral meniscus tears, 23 ACL injuries, 3 PCL injuries and 19 grade 2, 3 or 4 chondral defects (Table 2). The STARD patient flow diagram is shown in Figure 1.
Full size table
Full size table
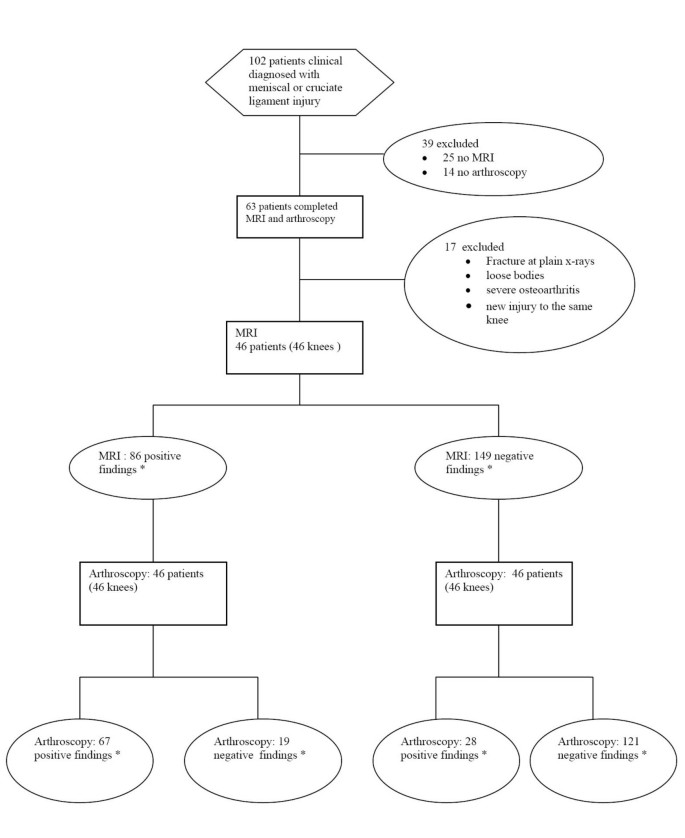
Standards for Reporting of Diagnostic Accuracy flow diagram. * Medial meniscus, lateral meniscus, Anetrior cruciate ligament, posterior cruciate ligament ruptures and chondral injuries.
Full size image
After the classification of the MRI diagnoses in true positive, false positive, true negative and false negative the accuracy, specificity, sensitivity, PPV, NPV, the LR+ and LR- and the AUC were calculated and are demonstrated in table 3. The sensitivity of MRI for medial meniscus rupture was 83% and the specificity 69%. The area under the ROC curve was 0.75. For ACL ruptures the percentage was higher with sensitivity reaching 83%, specificity 89% and area under the ROC 0.86 Slightly inferior were the results for lateral meniscus rupture with accuracy at 77%, sensitivity 62%, specificity 88% and AUC 0.75. Significantly inferior was the accuracy of MRI as far as the chondral defects concerns, with values of 60% in accuracy, 42% in sensitivity, 73% in specificity and AUC 0.57. We have separately evaluated the predictive value of clinical examination as far as the meniscal and anterior cruciate ligament injuries concern. Overall, clinical examination revealed 40 meniscus tears and 25 cruciate ligament injuries. Table 4 demonstrates results for the diagnostic value of the clinical examination obtained from this study.
Full size table
Full size table
Discussion
The purpose of this study was to demonstrate the diagnostic value of MRI in diagnosing the presence or absence of the most common injuries of the knee; the meniscus tears, the cruciate ligament ruptures and the chondral defects.
There are studies that support the view that the diagnostic accuracy of the MRI could affect in a critical way the treatment pathway of knee injuries. McKenzie et al [8] have studied 332 patients’ diagnosis before and after MRI. The diagnosis was initially based upon the clinical examination and the therapeutic procedure was decided before MRI. 57 from 113 clinically positive before MRI meniscal tears were not confirmed with MRI. This result leaded to revaluation and differentiation of treatment in 62% of the patients. From those patients programmed for surgery only 38% finally underwent arthroscopy. In another study, Weinstabl et al [9] randomly distributed patients with positive meniscus rupture tests in two groups. All the patients of the first group had MRI examination before arthroscopy. In this group only 2% of patients didn’t have positive findings during arthroscopy. Second group patients underwent arthroscopy, based only to the findings of the clinical examination. In this group, only in 30% of patients arthroscopy confirmed the findings of clinical examination.
However, in our study, MRI showed false results in significant proportion. For example as far as medial meniscus concerns there were 5 false positive and 5 false negative diagnosis whereas for lateral meniscus there were 8 false positive and 3 false negative diagnosis (PPV 83% and 81%, NPV 69% and 74% for medial and lateral meniscus tears respectively). As far as the chondral lesions concerns the MRI results were even more inferior with PPV and NPV reaching 53% and 63% respectively.
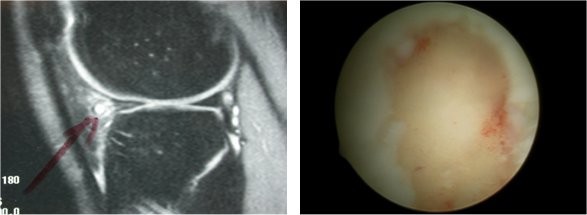
There are several explanations for the misleading results of MRI regarding the menisci. Firstly, meniscal tears and meniscus degenerative changes have the same appearance in MRI, by giving high signal within the meniscus [10]. Diagnosis then depends on the expansion of the high signal line towards meniscus articular surface [11] (FIGURE 2). Moreover, one of the most frequent causes for false positive MRI regarding the lateral meniscus is the misinterpretation of the signal coming from the inferior knee artery [12]. Helman et al [13] accredited in this structure about 38% of false positive MRI results. Often, the popliteal bursa or Humphrys’ ligament may mimic posterior lateral meniscus tears as well [14, 13]. McKenzie et al [15] summarized the four most common reasons for false positive diagnosis; wrong diagnosis due to variable anatomic structures, overestimation of pathology countered as meniscus tear (for example chondral injuries that mimic meniscus tears), false negative arthroscopic findings and tears within the meniscus without expansion to the articular surface. On the other hand the false negative results seem to occur exclusively from misinterpretation of MRI [16, 14, 1].
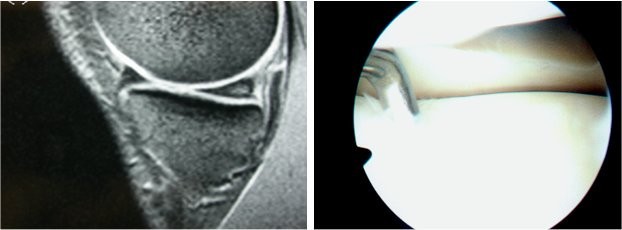
Left: Intrabody signal of the posterior aspect of meniscus, without extension to the articular surface. Right: At arthroscopy the meniscus appearance was normal.
Full size image
As far as the cruciate ligaments concerns, our study showed that from the 27 ACL ruptures diagnosed during arthroscopy 8 of them were missed by the MRI, leading to NPV of MRI for ACL ruptures of 86%. Causes of that target loss are easily recognized; firstly, in cases with ligament rupture without ligamentum mucosum rupture, MRI gives false negative results. Additionally, ruptures near ligaments’ insertion may be missed and MRI examination reveals an intact ACL. On contrary, false positive ACL ruptures occur in cases of intrabody mucosal or eosinophilic degeneration of the ACL [17, 18]. (FIGURE 3).
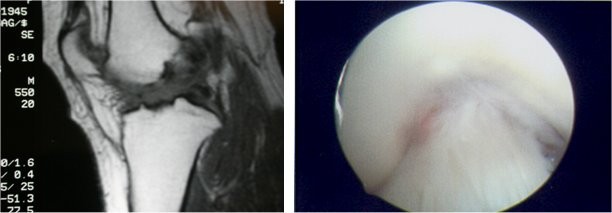
Left: Abnormal appearance of the ACL, suggesting a rupture. Right: At arthroscopy, the ACL appeared normal.
Full size image
The posterior cruciate ligament can be examined very well with MRI. Bibliography refers accuracy in ruptures higher than 90% [19, 20, 1]. In our study we evaluated only 3 PCL ruptures and all were identified by MRI. At the same time, one false positive result occurred (accuracy 98%, sensitivity 100%, specificity 98%). Even though our results agree with the bibliography data, the number of cases is too small for statistical significant conclusions. However, surgeons must always bear in mind that PCL is difficult to investigate during arthroscopy because of its anatomic position, and many times there are arthroscopic false negative results.
In this study, from 19 grade 2, 3 or 4 chondral defects (diameter >1 cm) diagnosed arthroscopically only 8 were preoperatively described in MRI (PPV 53%) and additionally, there were 7 false positive diagnosis. In total accuracy was 60%, sensitivity only 42% and specificity 73% (FIGURES 4, 5). In many cases, subchondral bone bruises that are frequently described in MRI, are mistaken with chondral defects, leading to false positive results (FIGURE 4). They remain though important cause of pain and morbidity. Additionally, one must never forget that preoperative MRI mainly focuses on meniscal and cruciate ligament injuries. As a result, chondral lesions are often underestimated and misdiagnosed by MRI [21, 22]. Postoperative new examination with MRI that focus on chondral defects leads to improvement of the diagnostic results [23, 21, 22].

Right: MRI suggesting damage at the articular cartilage. Left: At arthroscopy, the cartilage appeared normal.
Full size image
Left: Radiologist points out possible meniscal cyst. Right: At arthroscopy surgeon faced extensive articular cartilage damage.
Full size image
Other authors however, like Heron et al [24], have shown that MRI can satisfactory reveal the 2nd and 3rd grade chondral defects as well as damages at the patellar articular cartilage, but is not accurate for smaller injuries like fibrilization or small fissuring in articular hyaline cartilage. Similar results were reported from Ochi et al [23] who showed that the sensitivity of MRI increased (from 40% to 71%) when MRI reading was done retrospectively, after the arthroscopic findings were registered. Especially, in chondral lesions with full thickness loss of cartilage and large-deep erosions the retrospectively calculated MRI sensitivity was 100% and 75% respectively. On the other hand site surface injuries, fibrillization or shallow small cuts were not well described, not even post-arthroscopically. Furthermore, according to Mori et al [22], usage of modern, improved techniques, can not only reveal the size of chondral lesions but to distinguish partial from full depth chondral damages as well.
There is no doubt that the radiologist’s experience and training are very important factors in interpretation of MRI. At the same time reliable statistical data of the diagnostic value of MRI are also related with the independent base of reference. Regarding knee MRI, in most of the studies and in our study as well, the base of reference is arthroscopy. This presupposes that arthroscopy is 100% accurate and allows for the diagnosis of every possible knee pathology. This is not always the case [25, 16] ; arthroscopy is a technical demanding procedure and the results are varying according to surgeons’ experience, especially in difficult cases. From the 13 false positive results of our study, the majority referred to posterior meniscus tear. Nevertheless the belief is that, even in these cases, the meniscus pathology existed but failed to be discovered during arthroscopy [12, 26]. Especially the inferior surface of posterior aspect of the medial meniscus is difficult to be reached with a probe and often rupture at that point can be missed. Nowadays, the overall accuracy of arthroscopy varies between 70–100%, depending on the surgeons’ experience [16, 27–29]. This fluctuation inevitably raises questions, regarding the reliability of the MRI results classification on true or false [30].
In the everyday practice, based on clinical examination that comes first, surgeons decide whether must proceed to further laboratory tests, MRI, conservative or surgical treatment. But how precise can clinical examination be? There seems to be disagreement regarding the answer to this question. Investigations support that the accuracy of clinical examination compared with arthroscopic findings ranges between 64–85% [31, 32]. Rose et al [18] found that clinical examination is as accurate as MRI in diagnosing meniscal tears and ACL ruptures, so they concluded that MRI because of its high cost is not necessary in patients with clinical suspicion of meniscus and cruciate ligament tears. Similar conclusion was reported by Boden et al [33] who supported that when clinical examination sets the diagnosis of meniscus damage, MRI will not change treatment decisions.
On the other hand, Ruwe et at [34] reported that preoperative MRI can prevent unnecessary arthroscopy in 50% of the patients, so is of great value and must be done preoperatively. Boeree et al [35] believe that clinical examination is of minor significance with sensitivity in diagnosing medial meniscus, lateral meniscus and ACL tear of 67%, 48% and 55% respectively. Similar conclusions were reported by Jackson et al [36] who concluded that negative MRI for meniscus or cruciate ligament tears can discourage diagnostic arthroscopy even if clinical examination is positive for injury. The results of our study come in agreement with these studies, confirming a quite low diagnostic performance of the clinical examination (Table 4).
In summary, from our results, the accuracy of MRI in medial and lateral meniscus tear was 81% and 77% respectively, whilst for ACL and PCL rupture was 86% and 98% respectively. In the existing bibliography the accuracy of MRI reaches 90% in medial meniscus and ACL injuries, is lesser in lateral meniscus injury and slightly higher in PCL injuries [19, 26, 20, 37, 1, 38]. Most of the studies agree that MRI has low accuracy and sensitivity as far as chondral defects concerns [12, 23, 39]. The same has been shown in the current study, with the accuracy to be only 60% and the sensitivity and specificity 42% and 73% respectively.
It is true that our results have yield worst diagnostic value of MRI in comparison with the results of larger multicenter studies [1] and of large systematic reviews [40] (FIGURE 6). This can be attributed to the limitations of the current study, which is a retrospective non randomized study with relatively small number of patients. Especially, the patients with a PCL injury were too few, in order to draw significant results. However, it is our believe that our findings mirror the reality that the average Orthopaedic surgeon will face during his everyday clinical practice.
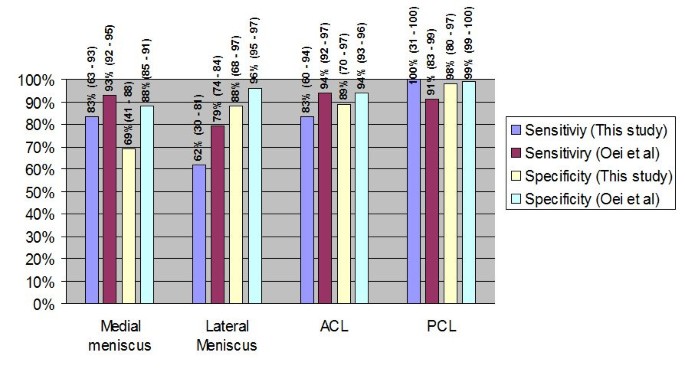
Comparison of the results (mean values and 95% confidence intervals) from this study compared with the results of the meta-analysis by Oei et al [40].
Full size image
Conclusion
In conclusion, the present study supports that MRI is very helpful in diagnosing meniscal and cruciate ligament injuries. But in a countable percentage reports with false results and in chondral defects its importance is still vague. Nowadays patients’ expectations are maximal and taking in account that MRI false or misleading results can be as high as 20% to 30% in specific knee pathologies it is concluded that arthroscopy still remains the gold standard in diagnosing the internal knee lesions. Undoubtedly new techniques and more powerful tomographers will improve MRI’s accuracy leading to better diagnostic equipment in knee injuries.
In any case, what one must always have in mind is that diagnosis alone is no the end point of the treatment and does not solve the problem. It is the beginning of new thoughts and actions one must follow to achieve accurate prognosis and correct treatment. In order to plan and apply the correct treatment pathways, the most important is not statistics or cost effectiveness data. Clinical experience and adequacy of the surgeon always have the greatest value, when it comes to the assurance of the patient optimal treatment.
References
-
Fischer SP, Fox JM, Del Pizzo W, Friedman MJ, Snyder SJ, Ferkel RD: Accuracy of diagnoses from magnetic resonance imaging of the knee. A multi-center analysis of one thousand and fourteen patients. J Bone Joint Surg Am. 1991, 73 (1): 2-10.
CAS
PubMedGoogle Scholar
-
Sherman OH, Fox JM, Snyder SJ, Del Pizzo W, Friedman MJ, Ferkel RD, Lawley MJ: Arthroscopy—«no-problem surgery». An analysis of complications in two thousand six hundred and forty cases. J Bone Joint Surg Am. 1986, 68 (2): 256-265.
CAS
PubMedGoogle Scholar
-
Lee JK, Yao L, Phelps CT, Wirth CR, Czajka J, Lozman J: Anterior cruciate ligament tears: MR imaging compared with arthroscopy and clinical tests. Radiology. 1988, 166 (3): 861-864.
Article
CAS
PubMedGoogle Scholar
-
Gelb HJ, Glasgow SG, Sapega AA, Torg JS: Magnetic resonance imaging of knee disorders. Clinical value and cost-effectiveness in a sports medicine practice. Am J Sports Med. 1996, 24 (1): 99-103. 10.1177/036354659602400118.
Article
CAS
PubMedGoogle Scholar
-
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig LM, Lijmer JG, Moher D, Rennie D, de Vet HC: Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative. BMJ. 2003, 326 (7379): 41-44. 10.1136/bmj.326.7379.41. 2003/01/04
Article
PubMed
PubMed CentralGoogle Scholar
-
Benjaminse A, Gokeler A, van der Schans CP: Clinical diagnosis of an anterior cruciate ligament rupture: a meta-analysis. J Orthop Sports Phys Ther. 2006, 36 (5): 267-288.
Article
PubMedGoogle Scholar
-
Outerbridge RE: The etiology of chondromalacia patellae. J Bone Joint Surg Br. 1961, 43-B: 752-757.
CAS
PubMedGoogle Scholar
-
Mackenzie R, Dixon AK, Keene GS, Hollingworth W, Lomas DJ, Villar RN: Magnetic resonance imaging of the knee: assessment of effectiveness. Clin Radiol. 1996, 51 (4): 245-250. 10.1016/S0009-9260(96)80340-0.
Article
CAS
PubMedGoogle Scholar
-
Weinstabl R, Muellner T, Vecsei V, Kainberger F, Kramer M: Economic considerations for the diagnosis and therapy of meniscal lesions: can magnetic resonance imaging help reduce the expense?. World J Surg. 1997, 21 (4): 363-368. 10.1007/PL00012254.
Article
CAS
PubMedGoogle Scholar
-
Dixon AK: Magnetic resonance imaging of meniscal tears of the knee. J Bone Joint Surg Br. 1996, 78 (2): 174-176.
CAS
PubMedGoogle Scholar
-
Tyrrell RL, Gluckert K, Pathria M, Modic MT: Fast three-dimensional MR imaging of the knee: comparison with arthroscopy. Radiology. 1988, 166 (3): 865-872.
Article
CAS
PubMedGoogle Scholar
-
Spiers AS, Meagher T, Ostlere SJ, Wilson DJ, Dodd CA: Can MRI of the knee affect arthroscopic practice? A prospective study of 58 patients. J Bone Joint Surg Br. 1993, 75 (1): 49-52.
CAS
PubMedGoogle Scholar
-
Herman LJ, Beltran J: Pitfalls in MR imaging of the knee. Radiology. 1988, 167 (3): 775-781.
Article
CAS
PubMedGoogle Scholar
-
Watanabe AT, Carter BC, Teitelbaum GP, Bradley WG: Common pitfalls in magnetic resonance imaging of the knee. J Bone Joint Surg Am. 1989, 71 (6): 857-862.
CAS
PubMedGoogle Scholar
-
Mackenzie R, Palmer CR, Lomas DJ, Dixon AK: Magnetic resonance imaging of the knee: diagnostic performance studies. Clin Radiol. 1996, 51 (4): 251-257. 10.1016/S0009-9260(96)80341-2.
Article
CAS
PubMedGoogle Scholar
-
Ireland J, Trickey EL, Stoker DJ: Arthroscopy and arthrography of the knee: a critical review. J Bone Joint Surg Br. 1980, 62-B (1): 3-6.
CAS
PubMedGoogle Scholar
-
Hodler J, Haghighi P, Trudell D, Resnick D: The cruciate ligaments of the knee: correlation between MR appearance and gross and histologic findings in cadaveric specimens. AJR Am J Roentgenol. 1992, 159 (2): 357-360.
Article
CAS
PubMedGoogle Scholar
-
Rose NE, Gold SM: A comparison of accuracy between clinical examination and magnetic resonance imaging in the diagnosis of meniscal and anterior cruciate ligament tears. Arthroscopy. 1996, 12 (4): 398-405.
Article
CAS
PubMedGoogle Scholar
-
Bassett LW, Grover JS, Seeger LL: Magnetic resonance imaging of knee trauma. Skeletal Radiol. 1990, 19 (6): 401-405. 10.1007/BF00241788.
Article
CAS
PubMedGoogle Scholar
-
Trieshmann HW, Mosure JC: The impact of magnetic resonance imaging of the knee on surgical decision making. Arthroscopy. 1996, 12 (5): 550-555.
Article
PubMedGoogle Scholar
-
Speer KP, Spritzer CE, Goldner JL, Garrett WE: Magnetic resonance imaging of traumatic knee articular cartilage injuries. Am J Sports Med. 1991, 19 (4): 396-402. 10.1177/036354659101900414.
Article
CAS
PubMedGoogle Scholar
-
Mori R, Ochi M, Sakai Y, Adachi N, Uchio Y: Clinical significance of magnetic resonance imaging (MRI) for focal chondral lesions. Magn Reson Imaging. 1999, 17 (8): 1135-1140. 10.1016/S0730-725X(99)00033-8.
Article
CAS
PubMedGoogle Scholar
-
Ochi M, Sumen Y, Kanda T, Ikuta Y, Itoh K: The diagnostic value and limitation of magnetic resonance imaging on chondral lesions in the knee joint. Arthroscopy. 1994, 10 (2): 176-183.
Article
CAS
PubMedGoogle Scholar
-
Heron CW, Calvert PT: Three-dimensional gradient-echo MR imaging of the knee: comparison with arthroscopy in 100 patients. Radiology. 1992, 183 (3): 839-844.
Article
CAS
PubMedGoogle Scholar
-
Quinn SF, Brown TF: Meniscal tears diagnosed with MR imaging versus arthroscopy: how reliable a standard is arthroscopy?. Radiology. 1991, 181 (3): 843-847.
Article
CAS
PubMedGoogle Scholar
-
Crues JV, Mink J, Levy TL, Lotysch M, Stoller DW: Meniscal tears of the knee: accuracy of MR imaging. Radiology. 1987, 164 (2): 445-448.
Article
PubMedGoogle Scholar
-
Dandy DJ, Jackson RW: The diagnosis of problems after meniscectomy. J Bone Joint Surg Br. 1975, 57 (3): 349-352.
CAS
PubMedGoogle Scholar
-
Jackson RW, Abe I: The role of arthroscopy in the management of disorders of the knee. An analysis of 200 consecutive examinations. J Bone Joint Surg Br. 1972, 54 (2): 310-322.
CAS
PubMedGoogle Scholar
-
Boeve BF, Davidson RA, Staab EV: Magnetic resonance imaging in the evaluation of knee injuries. South Med J. 1991, 84 (9): 1123-1127. 10.1097/00007611-199109000-00016.
Article
CAS
PubMedGoogle Scholar
-
Mackenzie R, Keene GS, Lomas DJ, Dixon AK: Errors at knee magnetic resonance imaging: true or false?. Br J Radiol. 1995, 68 (814): 1045-1051.
Article
CAS
PubMedGoogle Scholar
-
Gillies H, Seligson D: Precision in the diagnosis of meniscal lesions: a comparison of clinical evaluation, arthrography, and arthroscopy. J Bone Joint Surg Am. 1979, 61 (3): 343-346.
CAS
PubMedGoogle Scholar
-
Simonsen O, Jensen J, Mouritsen P, Lauritzen J: The accuracy of clinical examination of injury of the knee joint. Injury. 1984, 16 (2): 96-101. 10.1016/S0020-1383(84)80007-8.
Article
CAS
PubMedGoogle Scholar
-
Boden SD, Labropoulos PA, Vailas JC: MR scanning of the acutely injured knee: sensitive, but is it cost effective?. Arthroscopy. 1990, 6 (4): 306-310.
Article
CAS
PubMedGoogle Scholar
-
Ruwe PA, Wright J, Randall RL, Lynch JK, Jokl P, McCarthy S: Can MR imaging effectively replace diagnostic arthroscopy?. Radiology. 1992, 183 (2): 335-339.
Article
CAS
PubMedGoogle Scholar
-
Boeree NR, Watkinson AF, Ackroyd CE, Johnson C: Magnetic resonance imaging of meniscal and cruciate injuries of the knee. J Bone Joint Surg Br. 1991, 73 (3): 452-457.
CAS
PubMedGoogle Scholar
-
Jackson DW, Jennings LD, Maywood RM, Berger PE: Magnetic resonance imaging of the knee. Am J Sports Med. 1988, 16 (1): 29-38. 10.1177/036354658801600105.
Article
CAS
PubMedGoogle Scholar
-
Barry KP, Mesgarzadeh M, Triolo J, Moyer R, Tehranzadeh J, Bonakdarpour A: Accuracy of MRI patterns in evaluating anterior cruciate ligament tears. Skeletal Radiol. 1996, 25 (4): 365-370. 10.1007/s002560050096.
Article
CAS
PubMedGoogle Scholar
-
Justice WW, Quinn SF: Error patterns in the MR imaging evaluation of menisci of the knee. Radiology. 1995, 196 (3): 617-621.
Article
CAS
PubMedGoogle Scholar
-
Munk B, Madsen F, Lundorf E, Staunstrup H, Schmidt SA, Bolvig L, Hellfritzsch MB, Jensen J: Clinical magnetic resonance imaging and arthroscopic findings in knees: a comparative prospective study of meniscus anterior cruciate ligament and cartilage lesions. Arthroscopy. 1998, 14 (2): 171-175.
Article
CAS
PubMedGoogle Scholar
-
Oei EH, Nikken JJ, Verstijnen AC, Ginai AZ, Myriam Hunink MG: MR imaging of the menisci and cruciate ligaments: a systematic review. Radiology. 2003, 226 (3): 837-848. 10.1148/radiol.2263011892. 2003/02/26
Article
PubMedGoogle Scholar
Download references
Acknowledgements
Funding was neither sought nor obtained.
Author information
Authors and Affiliations
-
Academic Department of Trauma & Orthopaedics, Leeds Teaching Hospitals, School of Medicine, University of Leeds, UK
Vassilios S Nikolaou & Peter Giannoudis
-
2nd Academic Department of Trauma & Orthopaedics, Konstantopoulion Hospital, Athens University, Greece
Efstathios Chronopoulos, Christianna Savvidou, Spyros Plessas, Nicolas Efstathopoulos & Georgios Papachristou
Authors
- Vassilios S Nikolaou
You can also search for this author in
PubMed Google Scholar - Efstathios Chronopoulos
You can also search for this author in
PubMed Google Scholar - Christianna Savvidou
You can also search for this author in
PubMed Google Scholar - Spyros Plessas
You can also search for this author in
PubMed Google Scholar - Peter Giannoudis
You can also search for this author in
PubMed Google Scholar - Nicolas Efstathopoulos
You can also search for this author in
PubMed Google Scholar - Georgios Papachristou
You can also search for this author in
PubMed Google Scholar
Corresponding author
Correspondence to
Vassilios S Nikolaou.
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
VN, CS and EC were involved in collecting patient details, reviewing the literature, drafted and proof read the manuscript, PG and NE were involved in drafted and proof read the manuscript, SP was involved in the operation of patients and registered the clinical findings, GP is the senior author and was responsible for final proof reading of the article. All authors have read and approved the final manuscript.
Authors’ original submitted files for images
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Reprints and Permissions
About this article
Cite this article
Nikolaou, V.S., Chronopoulos, E., Savvidou, C. et al. MRI efficacy in diagnosing internal lesions of the knee: a retrospective analysis.
J Trauma Manage Outcomes 2, 4 (2008). https://doi.org/10.1186/1752-2897-2-4
Download citation
-
Received: 23 February 2008
-
Accepted: 02 June 2008
-
Published: 02 June 2008
-
DOI: https://doi.org/10.1186/1752-2897-2-4
Keywords
- Positive Predictive Value
- Cruciate Ligament
- Posterior Cruciate Ligament
- Lateral Meniscus
- Medial Meniscus
- Research
- Open Access
- Published: 02 June 2008
- Efstathios Chronopoulos2,
- Christianna Savvidou2,
- Spyros Plessas2,
- Peter Giannoudis1,
- Nicolas Efstathopoulos2 &
- …
- Georgios Papachristou2
Journal of Trauma Management & Outcomes
volume 2, Article number: 4 (2008)
Cite this article
-
17k Accesses
-
45 Citations
-
11 Altmetric
-
Metrics details
Abstract
Background
Many surgeons tend to believe that MRI is an accurate, non invasive diagnostic method, enough to lead to decisions for conservative treatment and save a patient from unnecessary arthroscopy. We conducted a retrospective study to investigate the accuracy of the MRI of the knee for the detection of injuries of the meniscus, cruciate ligaments and articular cartilage, in comparison with the preoperative clinical examination and intraoperative findings. Between May 2005 and February 2006 102 patients after clinical examination were diagnosed with meniscal or cruciate injury and underwent definitive treatment with arthroscopy. 46 of these patients fulfilled the inclusion criteria. The accuracy, sensitivity, specificity, negative and positive predictive values of the MRI findings were correlated with the lesions identified during arthroscopy. The diagnostic performance of the initial clinical examination was also calculated for the meniscal and cruciate ligament injuries.
Results
The accuracy for tears of the medial, lateral meniscus, anterior and posterior cruciate ligaments and articular cartilage was 81%, 77%, 86%, 98% and 60% respectively. The specificity was 69%, 88%, 89%, 98% and 73% respectively. The positive predictive value was 83%, 81%, 90%, 75% and 53% respectively. Finally, the clinical examination had significant lower reliability in the detection of these injuries.
Conclusion
MRI is very helpful in diagnosing meniscal and cruciate ligament injuries. But in a countable percentage reports with false results and in chondral defects its importance is still vague. The arthroscopy still remains the gold standard for definitive diagnosis.
Peer Review reports
Background
Arthroscopy is considered as «the gold standard» for diagnosis of traumatic intraarticular knee lesions [1]. However, arthroscopy is an invasive procedure that requires hospitalization and anaesthesia, thus presenting all the potential complications of a surgical procedure [2]. Since it’s introduction in the 1980’s Magnetic Resonance Imaging (MRI) has gained in popularity as a diagnostic tool of the musculoskeletal disorders [3]. Especially the knee is the most frequent examined joint with MRI. Many surgeons tend to believe that MRI is an accurate, non invasive diagnostic method of the knee injuries, enough to lead to decisions for conservative treatment and save a patient from unnecessary arthroscopy. Nevertheless, even nowadays, remains very expensive. Taking in account that health-economics play important role in patients management, many questions arise regarding when and how often one must ask for an MRI when clinical examination has already confirm the diagnosis of meniscal tear or cruciate ligament rupture [4]. The opposite question might be more important; is negative MRI enough to prevent unnecessary arthroscopy, when clinical examination suggests a meniscal or cruciate ligament injury?
With the purpose of investigating the accuracy of magnetic resonance imaging in patients with clinical signs of traumatic intraarticular knee lesions, we compared its findings with those obtained from the subsequent arthroscopies.
Methods
After obtaining the approval of the hospital ethics committee, we retrospectively reviewed the case notes of patients who had been clinically diagnosed with meniscal or cruciate injury, between May 2005 and February 2006 in our institution. Patients who had subsequently undergone further examination with MRI and were definitively treated with arthroscopy were then identified. We adhered to the Standards for Reporting of Diagnostic Accuracy (STARD) criteria for design and presentation of diagnostic studies [5]
Patients that in plain X-rays had fractures, loose bodies or signs of severe osteoarthritis were excluded from the study. Additionally, patients that after the MRI examination have had new injury to the same knee, before the arthroscopy or delayed to undergo arthroscopy for more than 3 months, were also excluded.
All patients had thorough clinical examination from two experienced knee surgeons prior to the MRI. Clinical examination focused on meniscal injury and cruciate ligament injury. The tests used in the clinical diagnosis were: the anterior-posterior drawer test, the Lachman test, the pivot shift test for the diagnosis of cruciate ligament injuries and the Apley’s and McMurray’s test for the meniscal injuries [6].
MRI examinations were performed in 2 different diagnostic centres. The MRI scanners were two 1.5 tesla units (Philips Medical Systems). T1 and T2 weighted images in coronal, axial and sagittal planes were obtained. Slice thickness ranged from 3 to 5 mm. The films were interpreted from 2 experienced knee radiologists who were aware of the result of the clinical examination as this was written at the initial referral letter. Any abnormalities of the cruciate ligaments, menisci or hyaline cartilage were described on a standard form. Preoperatively each MRI was also assessed by the surgeon performing the arthroscopy. In the case of different opinions between the two, the radiologists’ diagnosis was considered more reliable.
All arthroscopies were performed by 2 experienced knee surgeons in a hospital environment with complete preoperative and postoperative care. A 4 mm Karl-Storz arthroscope with a 30-degree angle was used. Standard arthroscopic portals were used. ; the inferolateral portal for the arthroscope, and the inferomedial portal for the probe. Before any intervention, all knee interior structures were examined with the probe. Chondral defects were classified as positive if were more than 2nd grade according to the Outerbridge classification [7] and measured more than 1 cm in diameter. A cruciate ligament was considered to be torn if it was completely disrupted at one of its attachments to bone or in its substance, or if laxity (partial tear) could be demonstrated with a probe. All arthroscopic findings were photographed and registered. For further evaluation all arthroscopic findings were considered accurate and served as reference base.
MRI diagnoses and clinical findings were placed into one of four categories after arthroscopic evaluation. A result was considered a true-positive if the clinical or MRI diagnosis was confirmed by arthroscopic evaluation. A result was considered a true-negative if the diagnosis of no tears was confirmed by arthroscopy. A result was considered a false-positive if the arthroscopy was negative but the results were positive at the clinical examination or on the MRI. If the arthroscopy was positive but the clinical examination and MRI were negative, this was considered a false-negative result.
Statistical analysis was used to calculate sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV), in order to assess the realibility of the clinical and MRI results. 95% confidence intervals for sensitivity and specificity, as well as positive (LR+) and negative likelihood ratios (LR-) and areas under the ROC curve (AUC) were calculated.
Results
One hundred two patients after clinical examination were diagnosed with meniscal or cruciate injury and underwent definitive treatment with arthroscopy, during the studied period. After the application of the exclusion criteria we were able to identify 46 patients (30 males) that were further examined with MRI preoperatively. The mean age was 32 (18 – 45) years. Right knee injury presented to 21 whereas left knee injury to 25 patients. Table 1 summarizes the patients’ demographics. Arthroscopy revealed 33 medial meniscus tears, 21 lateral meniscus tears, 23 ACL injuries, 3 PCL injuries and 19 grade 2, 3 or 4 chondral defects (Table 2). The STARD patient flow diagram is shown in Figure 1.
Full size table
Full size table
Standards for Reporting of Diagnostic Accuracy flow diagram. * Medial meniscus, lateral meniscus, Anetrior cruciate ligament, posterior cruciate ligament ruptures and chondral injuries.
Full size image
After the classification of the MRI diagnoses in true positive, false positive, true negative and false negative the accuracy, specificity, sensitivity, PPV, NPV, the LR+ and LR- and the AUC were calculated and are demonstrated in table 3. The sensitivity of MRI for medial meniscus rupture was 83% and the specificity 69%. The area under the ROC curve was 0.75. For ACL ruptures the percentage was higher with sensitivity reaching 83%, specificity 89% and area under the ROC 0.86 Slightly inferior were the results for lateral meniscus rupture with accuracy at 77%, sensitivity 62%, specificity 88% and AUC 0.75. Significantly inferior was the accuracy of MRI as far as the chondral defects concerns, with values of 60% in accuracy, 42% in sensitivity, 73% in specificity and AUC 0.57. We have separately evaluated the predictive value of clinical examination as far as the meniscal and anterior cruciate ligament injuries concern. Overall, clinical examination revealed 40 meniscus tears and 25 cruciate ligament injuries. Table 4 demonstrates results for the diagnostic value of the clinical examination obtained from this study.
Full size table
Full size table
Discussion
The purpose of this study was to demonstrate the diagnostic value of MRI in diagnosing the presence or absence of the most common injuries of the knee; the meniscus tears, the cruciate ligament ruptures and the chondral defects.
There are studies that support the view that the diagnostic accuracy of the MRI could affect in a critical way the treatment pathway of knee injuries. McKenzie et al [8] have studied 332 patients’ diagnosis before and after MRI. The diagnosis was initially based upon the clinical examination and the therapeutic procedure was decided before MRI. 57 from 113 clinically positive before MRI meniscal tears were not confirmed with MRI. This result leaded to revaluation and differentiation of treatment in 62% of the patients. From those patients programmed for surgery only 38% finally underwent arthroscopy. In another study, Weinstabl et al [9] randomly distributed patients with positive meniscus rupture tests in two groups. All the patients of the first group had MRI examination before arthroscopy. In this group only 2% of patients didn’t have positive findings during arthroscopy. Second group patients underwent arthroscopy, based only to the findings of the clinical examination. In this group, only in 30% of patients arthroscopy confirmed the findings of clinical examination.
However, in our study, MRI showed false results in significant proportion. For example as far as medial meniscus concerns there were 5 false positive and 5 false negative diagnosis whereas for lateral meniscus there were 8 false positive and 3 false negative diagnosis (PPV 83% and 81%, NPV 69% and 74% for medial and lateral meniscus tears respectively). As far as the chondral lesions concerns the MRI results were even more inferior with PPV and NPV reaching 53% and 63% respectively.
There are several explanations for the misleading results of MRI regarding the menisci. Firstly, meniscal tears and meniscus degenerative changes have the same appearance in MRI, by giving high signal within the meniscus [10]. Diagnosis then depends on the expansion of the high signal line towards meniscus articular surface [11] (FIGURE 2). Moreover, one of the most frequent causes for false positive MRI regarding the lateral meniscus is the misinterpretation of the signal coming from the inferior knee artery [12]. Helman et al [13] accredited in this structure about 38% of false positive MRI results. Often, the popliteal bursa or Humphrys’ ligament may mimic posterior lateral meniscus tears as well [14, 13]. McKenzie et al [15] summarized the four most common reasons for false positive diagnosis; wrong diagnosis due to variable anatomic structures, overestimation of pathology countered as meniscus tear (for example chondral injuries that mimic meniscus tears), false negative arthroscopic findings and tears within the meniscus without expansion to the articular surface. On the other hand the false negative results seem to occur exclusively from misinterpretation of MRI [16, 14, 1].
Left: Intrabody signal of the posterior aspect of meniscus, without extension to the articular surface. Right: At arthroscopy the meniscus appearance was normal.
Full size image
As far as the cruciate ligaments concerns, our study showed that from the 27 ACL ruptures diagnosed during arthroscopy 8 of them were missed by the MRI, leading to NPV of MRI for ACL ruptures of 86%. Causes of that target loss are easily recognized; firstly, in cases with ligament rupture without ligamentum mucosum rupture, MRI gives false negative results. Additionally, ruptures near ligaments’ insertion may be missed and MRI examination reveals an intact ACL. On contrary, false positive ACL ruptures occur in cases of intrabody mucosal or eosinophilic degeneration of the ACL [17, 18]. (FIGURE 3).
Left: Abnormal appearance of the ACL, suggesting a rupture. Right: At arthroscopy, the ACL appeared normal.
Full size image
The posterior cruciate ligament can be examined very well with MRI. Bibliography refers accuracy in ruptures higher than 90% [19, 20, 1]. In our study we evaluated only 3 PCL ruptures and all were identified by MRI. At the same time, one false positive result occurred (accuracy 98%, sensitivity 100%, specificity 98%). Even though our results agree with the bibliography data, the number of cases is too small for statistical significant conclusions. However, surgeons must always bear in mind that PCL is difficult to investigate during arthroscopy because of its anatomic position, and many times there are arthroscopic false negative results.
In this study, from 19 grade 2, 3 or 4 chondral defects (diameter >1 cm) diagnosed arthroscopically only 8 were preoperatively described in MRI (PPV 53%) and additionally, there were 7 false positive diagnosis. In total accuracy was 60%, sensitivity only 42% and specificity 73% (FIGURES 4, 5). In many cases, subchondral bone bruises that are frequently described in MRI, are mistaken with chondral defects, leading to false positive results (FIGURE 4). They remain though important cause of pain and morbidity. Additionally, one must never forget that preoperative MRI mainly focuses on meniscal and cruciate ligament injuries. As a result, chondral lesions are often underestimated and misdiagnosed by MRI [21, 22]. Postoperative new examination with MRI that focus on chondral defects leads to improvement of the diagnostic results [23, 21, 22].
Right: MRI suggesting damage at the articular cartilage. Left: At arthroscopy, the cartilage appeared normal.
Full size image
Left: Radiologist points out possible meniscal cyst. Right: At arthroscopy surgeon faced extensive articular cartilage damage.
Full size image
Other authors however, like Heron et al [24], have shown that MRI can satisfactory reveal the 2nd and 3rd grade chondral defects as well as damages at the patellar articular cartilage, but is not accurate for smaller injuries like fibrilization or small fissuring in articular hyaline cartilage. Similar results were reported from Ochi et al [23] who showed that the sensitivity of MRI increased (from 40% to 71%) when MRI reading was done retrospectively, after the arthroscopic findings were registered. Especially, in chondral lesions with full thickness loss of cartilage and large-deep erosions the retrospectively calculated MRI sensitivity was 100% and 75% respectively. On the other hand site surface injuries, fibrillization or shallow small cuts were not well described, not even post-arthroscopically. Furthermore, according to Mori et al [22], usage of modern, improved techniques, can not only reveal the size of chondral lesions but to distinguish partial from full depth chondral damages as well.
There is no doubt that the radiologist’s experience and training are very important factors in interpretation of MRI. At the same time reliable statistical data of the diagnostic value of MRI are also related with the independent base of reference. Regarding knee MRI, in most of the studies and in our study as well, the base of reference is arthroscopy. This presupposes that arthroscopy is 100% accurate and allows for the diagnosis of every possible knee pathology. This is not always the case [25, 16] ; arthroscopy is a technical demanding procedure and the results are varying according to surgeons’ experience, especially in difficult cases. From the 13 false positive results of our study, the majority referred to posterior meniscus tear. Nevertheless the belief is that, even in these cases, the meniscus pathology existed but failed to be discovered during arthroscopy [12, 26]. Especially the inferior surface of posterior aspect of the medial meniscus is difficult to be reached with a probe and often rupture at that point can be missed. Nowadays, the overall accuracy of arthroscopy varies between 70–100%, depending on the surgeons’ experience [16, 27–29]. This fluctuation inevitably raises questions, regarding the reliability of the MRI results classification on true or false [30].
In the everyday practice, based on clinical examination that comes first, surgeons decide whether must proceed to further laboratory tests, MRI, conservative or surgical treatment. But how precise can clinical examination be? There seems to be disagreement regarding the answer to this question. Investigations support that the accuracy of clinical examination compared with arthroscopic findings ranges between 64–85% [31, 32]. Rose et al [18] found that clinical examination is as accurate as MRI in diagnosing meniscal tears and ACL ruptures, so they concluded that MRI because of its high cost is not necessary in patients with clinical suspicion of meniscus and cruciate ligament tears. Similar conclusion was reported by Boden et al [33] who supported that when clinical examination sets the diagnosis of meniscus damage, MRI will not change treatment decisions.
On the other hand, Ruwe et at [34] reported that preoperative MRI can prevent unnecessary arthroscopy in 50% of the patients, so is of great value and must be done preoperatively. Boeree et al [35] believe that clinical examination is of minor significance with sensitivity in diagnosing medial meniscus, lateral meniscus and ACL tear of 67%, 48% and 55% respectively. Similar conclusions were reported by Jackson et al [36] who concluded that negative MRI for meniscus or cruciate ligament tears can discourage diagnostic arthroscopy even if clinical examination is positive for injury. The results of our study come in agreement with these studies, confirming a quite low diagnostic performance of the clinical examination (Table 4).
In summary, from our results, the accuracy of MRI in medial and lateral meniscus tear was 81% and 77% respectively, whilst for ACL and PCL rupture was 86% and 98% respectively. In the existing bibliography the accuracy of MRI reaches 90% in medial meniscus and ACL injuries, is lesser in lateral meniscus injury and slightly higher in PCL injuries [19, 26, 20, 37, 1, 38]. Most of the studies agree that MRI has low accuracy and sensitivity as far as chondral defects concerns [12, 23, 39]. The same has been shown in the current study, with the accuracy to be only 60% and the sensitivity and specificity 42% and 73% respectively.
It is true that our results have yield worst diagnostic value of MRI in comparison with the results of larger multicenter studies [1] and of large systematic reviews [40] (FIGURE 6). This can be attributed to the limitations of the current study, which is a retrospective non randomized study with relatively small number of patients. Especially, the patients with a PCL injury were too few, in order to draw significant results. However, it is our believe that our findings mirror the reality that the average Orthopaedic surgeon will face during his everyday clinical practice.
Comparison of the results (mean values and 95% confidence intervals) from this study compared with the results of the meta-analysis by Oei et al [40].
Full size image
Conclusion
In conclusion, the present study supports that MRI is very helpful in diagnosing meniscal and cruciate ligament injuries. But in a countable percentage reports with false results and in chondral defects its importance is still vague. Nowadays patients’ expectations are maximal and taking in account that MRI false or misleading results can be as high as 20% to 30% in specific knee pathologies it is concluded that arthroscopy still remains the gold standard in diagnosing the internal knee lesions. Undoubtedly new techniques and more powerful tomographers will improve MRI’s accuracy leading to better diagnostic equipment in knee injuries.
In any case, what one must always have in mind is that diagnosis alone is no the end point of the treatment and does not solve the problem. It is the beginning of new thoughts and actions one must follow to achieve accurate prognosis and correct treatment. In order to plan and apply the correct treatment pathways, the most important is not statistics or cost effectiveness data. Clinical experience and adequacy of the surgeon always have the greatest value, when it comes to the assurance of the patient optimal treatment.
References
-
Fischer SP, Fox JM, Del Pizzo W, Friedman MJ, Snyder SJ, Ferkel RD: Accuracy of diagnoses from magnetic resonance imaging of the knee. A multi-center analysis of one thousand and fourteen patients. J Bone Joint Surg Am. 1991, 73 (1): 2-10.
CAS
PubMedGoogle Scholar
-
Sherman OH, Fox JM, Snyder SJ, Del Pizzo W, Friedman MJ, Ferkel RD, Lawley MJ: Arthroscopy—«no-problem surgery». An analysis of complications in two thousand six hundred and forty cases. J Bone Joint Surg Am. 1986, 68 (2): 256-265.
CAS
PubMedGoogle Scholar
-
Lee JK, Yao L, Phelps CT, Wirth CR, Czajka J, Lozman J: Anterior cruciate ligament tears: MR imaging compared with arthroscopy and clinical tests. Radiology. 1988, 166 (3): 861-864.
Article
CAS
PubMedGoogle Scholar
-
Gelb HJ, Glasgow SG, Sapega AA, Torg JS: Magnetic resonance imaging of knee disorders. Clinical value and cost-effectiveness in a sports medicine practice. Am J Sports Med. 1996, 24 (1): 99-103. 10.1177/036354659602400118.
Article
CAS
PubMedGoogle Scholar
-
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig LM, Lijmer JG, Moher D, Rennie D, de Vet HC: Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative. BMJ. 2003, 326 (7379): 41-44. 10.1136/bmj.326.7379.41. 2003/01/04
Article
PubMed
PubMed CentralGoogle Scholar
-
Benjaminse A, Gokeler A, van der Schans CP: Clinical diagnosis of an anterior cruciate ligament rupture: a meta-analysis. J Orthop Sports Phys Ther. 2006, 36 (5): 267-288.
Article
PubMedGoogle Scholar
-
Outerbridge RE: The etiology of chondromalacia patellae. J Bone Joint Surg Br. 1961, 43-B: 752-757.
CAS
PubMedGoogle Scholar
-
Mackenzie R, Dixon AK, Keene GS, Hollingworth W, Lomas DJ, Villar RN: Magnetic resonance imaging of the knee: assessment of effectiveness. Clin Radiol. 1996, 51 (4): 245-250. 10.1016/S0009-9260(96)80340-0.
Article
CAS
PubMedGoogle Scholar
-
Weinstabl R, Muellner T, Vecsei V, Kainberger F, Kramer M: Economic considerations for the diagnosis and therapy of meniscal lesions: can magnetic resonance imaging help reduce the expense?. World J Surg. 1997, 21 (4): 363-368. 10.1007/PL00012254.
Article
CAS
PubMedGoogle Scholar
-
Dixon AK: Magnetic resonance imaging of meniscal tears of the knee. J Bone Joint Surg Br. 1996, 78 (2): 174-176.
CAS
PubMedGoogle Scholar
-
Tyrrell RL, Gluckert K, Pathria M, Modic MT: Fast three-dimensional MR imaging of the knee: comparison with arthroscopy. Radiology. 1988, 166 (3): 865-872.
Article
CAS
PubMedGoogle Scholar
-
Spiers AS, Meagher T, Ostlere SJ, Wilson DJ, Dodd CA: Can MRI of the knee affect arthroscopic practice? A prospective study of 58 patients. J Bone Joint Surg Br. 1993, 75 (1): 49-52.
CAS
PubMedGoogle Scholar
-
Herman LJ, Beltran J: Pitfalls in MR imaging of the knee. Radiology. 1988, 167 (3): 775-781.
Article
CAS
PubMedGoogle Scholar
-
Watanabe AT, Carter BC, Teitelbaum GP, Bradley WG: Common pitfalls in magnetic resonance imaging of the knee. J Bone Joint Surg Am. 1989, 71 (6): 857-862.
CAS
PubMedGoogle Scholar
-
Mackenzie R, Palmer CR, Lomas DJ, Dixon AK: Magnetic resonance imaging of the knee: diagnostic performance studies. Clin Radiol. 1996, 51 (4): 251-257. 10.1016/S0009-9260(96)80341-2.
Article
CAS
PubMedGoogle Scholar
-
Ireland J, Trickey EL, Stoker DJ: Arthroscopy and arthrography of the knee: a critical review. J Bone Joint Surg Br. 1980, 62-B (1): 3-6.
CAS
PubMedGoogle Scholar
-
Hodler J, Haghighi P, Trudell D, Resnick D: The cruciate ligaments of the knee: correlation between MR appearance and gross and histologic findings in cadaveric specimens. AJR Am J Roentgenol. 1992, 159 (2): 357-360.
Article
CAS
PubMedGoogle Scholar
-
Rose NE, Gold SM: A comparison of accuracy between clinical examination and magnetic resonance imaging in the diagnosis of meniscal and anterior cruciate ligament tears. Arthroscopy. 1996, 12 (4): 398-405.
Article
CAS
PubMedGoogle Scholar
-
Bassett LW, Grover JS, Seeger LL: Magnetic resonance imaging of knee trauma. Skeletal Radiol. 1990, 19 (6): 401-405. 10.1007/BF00241788.
Article
CAS
PubMedGoogle Scholar
-
Trieshmann HW, Mosure JC: The impact of magnetic resonance imaging of the knee on surgical decision making. Arthroscopy. 1996, 12 (5): 550-555.
Article
PubMedGoogle Scholar
-
Speer KP, Spritzer CE, Goldner JL, Garrett WE: Magnetic resonance imaging of traumatic knee articular cartilage injuries. Am J Sports Med. 1991, 19 (4): 396-402. 10.1177/036354659101900414.
Article
CAS
PubMedGoogle Scholar
-
Mori R, Ochi M, Sakai Y, Adachi N, Uchio Y: Clinical significance of magnetic resonance imaging (MRI) for focal chondral lesions. Magn Reson Imaging. 1999, 17 (8): 1135-1140. 10.1016/S0730-725X(99)00033-8.
Article
CAS
PubMedGoogle Scholar
-
Ochi M, Sumen Y, Kanda T, Ikuta Y, Itoh K: The diagnostic value and limitation of magnetic resonance imaging on chondral lesions in the knee joint. Arthroscopy. 1994, 10 (2): 176-183.
Article
CAS
PubMedGoogle Scholar
-
Heron CW, Calvert PT: Three-dimensional gradient-echo MR imaging of the knee: comparison with arthroscopy in 100 patients. Radiology. 1992, 183 (3): 839-844.
Article
CAS
PubMedGoogle Scholar
-
Quinn SF, Brown TF: Meniscal tears diagnosed with MR imaging versus arthroscopy: how reliable a standard is arthroscopy?. Radiology. 1991, 181 (3): 843-847.
Article
CAS
PubMedGoogle Scholar
-
Crues JV, Mink J, Levy TL, Lotysch M, Stoller DW: Meniscal tears of the knee: accuracy of MR imaging. Radiology. 1987, 164 (2): 445-448.
Article
PubMedGoogle Scholar
-
Dandy DJ, Jackson RW: The diagnosis of problems after meniscectomy. J Bone Joint Surg Br. 1975, 57 (3): 349-352.
CAS
PubMedGoogle Scholar
-
Jackson RW, Abe I: The role of arthroscopy in the management of disorders of the knee. An analysis of 200 consecutive examinations. J Bone Joint Surg Br. 1972, 54 (2): 310-322.
CAS
PubMedGoogle Scholar
-
Boeve BF, Davidson RA, Staab EV: Magnetic resonance imaging in the evaluation of knee injuries. South Med J. 1991, 84 (9): 1123-1127. 10.1097/00007611-199109000-00016.
Article
CAS
PubMedGoogle Scholar
-
Mackenzie R, Keene GS, Lomas DJ, Dixon AK: Errors at knee magnetic resonance imaging: true or false?. Br J Radiol. 1995, 68 (814): 1045-1051.
Article
CAS
PubMedGoogle Scholar
-
Gillies H, Seligson D: Precision in the diagnosis of meniscal lesions: a comparison of clinical evaluation, arthrography, and arthroscopy. J Bone Joint Surg Am. 1979, 61 (3): 343-346.
CAS
PubMedGoogle Scholar
-
Simonsen O, Jensen J, Mouritsen P, Lauritzen J: The accuracy of clinical examination of injury of the knee joint. Injury. 1984, 16 (2): 96-101. 10.1016/S0020-1383(84)80007-8.
Article
CAS
PubMedGoogle Scholar
-
Boden SD, Labropoulos PA, Vailas JC: MR scanning of the acutely injured knee: sensitive, but is it cost effective?. Arthroscopy. 1990, 6 (4): 306-310.
Article
CAS
PubMedGoogle Scholar
-
Ruwe PA, Wright J, Randall RL, Lynch JK, Jokl P, McCarthy S: Can MR imaging effectively replace diagnostic arthroscopy?. Radiology. 1992, 183 (2): 335-339.
Article
CAS
PubMedGoogle Scholar
-
Boeree NR, Watkinson AF, Ackroyd CE, Johnson C: Magnetic resonance imaging of meniscal and cruciate injuries of the knee. J Bone Joint Surg Br. 1991, 73 (3): 452-457.
CAS
PubMedGoogle Scholar
-
Jackson DW, Jennings LD, Maywood RM, Berger PE: Magnetic resonance imaging of the knee. Am J Sports Med. 1988, 16 (1): 29-38. 10.1177/036354658801600105.
Article
CAS
PubMedGoogle Scholar
-
Barry KP, Mesgarzadeh M, Triolo J, Moyer R, Tehranzadeh J, Bonakdarpour A: Accuracy of MRI patterns in evaluating anterior cruciate ligament tears. Skeletal Radiol. 1996, 25 (4): 365-370. 10.1007/s002560050096.
Article
CAS
PubMedGoogle Scholar
-
Justice WW, Quinn SF: Error patterns in the MR imaging evaluation of menisci of the knee. Radiology. 1995, 196 (3): 617-621.
Article
CAS
PubMedGoogle Scholar
-
Munk B, Madsen F, Lundorf E, Staunstrup H, Schmidt SA, Bolvig L, Hellfritzsch MB, Jensen J: Clinical magnetic resonance imaging and arthroscopic findings in knees: a comparative prospective study of meniscus anterior cruciate ligament and cartilage lesions. Arthroscopy. 1998, 14 (2): 171-175.
Article
CAS
PubMedGoogle Scholar
-
Oei EH, Nikken JJ, Verstijnen AC, Ginai AZ, Myriam Hunink MG: MR imaging of the menisci and cruciate ligaments: a systematic review. Radiology. 2003, 226 (3): 837-848. 10.1148/radiol.2263011892. 2003/02/26
Article
PubMedGoogle Scholar
Download references
Acknowledgements
Funding was neither sought nor obtained.
Author information
Authors and Affiliations
-
Academic Department of Trauma & Orthopaedics, Leeds Teaching Hospitals, School of Medicine, University of Leeds, UK
Vassilios S Nikolaou & Peter Giannoudis
-
2nd Academic Department of Trauma & Orthopaedics, Konstantopoulion Hospital, Athens University, Greece
Efstathios Chronopoulos, Christianna Savvidou, Spyros Plessas, Nicolas Efstathopoulos & Georgios Papachristou
Authors
- Vassilios S Nikolaou
You can also search for this author in
PubMed Google Scholar - Efstathios Chronopoulos
You can also search for this author in
PubMed Google Scholar - Christianna Savvidou
You can also search for this author in
PubMed Google Scholar - Spyros Plessas
You can also search for this author in
PubMed Google Scholar - Peter Giannoudis
You can also search for this author in
PubMed Google Scholar - Nicolas Efstathopoulos
You can also search for this author in
PubMed Google Scholar - Georgios Papachristou
You can also search for this author in
PubMed Google Scholar
Corresponding author
Correspondence to
Vassilios S Nikolaou.
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
VN, CS and EC were involved in collecting patient details, reviewing the literature, drafted and proof read the manuscript, PG and NE were involved in drafted and proof read the manuscript, SP was involved in the operation of patients and registered the clinical findings, GP is the senior author and was responsible for final proof reading of the article. All authors have read and approved the final manuscript.
Authors’ original submitted files for images
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Reprints and Permissions
About this article
Cite this article
Nikolaou, V.S., Chronopoulos, E., Savvidou, C. et al. MRI efficacy in diagnosing internal lesions of the knee: a retrospective analysis.
J Trauma Manage Outcomes 2, 4 (2008). https://doi.org/10.1186/1752-2897-2-4
Download citation
-
Received: 23 February 2008
-
Accepted: 02 June 2008
-
Published: 02 June 2008
-
DOI: https://doi.org/10.1186/1752-2897-2-4
Keywords
- Positive Predictive Value
- Cruciate Ligament
- Posterior Cruciate Ligament
- Lateral Meniscus
- Medial Meniscus
МРТ коленного сустава – это современный неинвазивный метод обследования, часто применяемый в травматологии и ортопедии. С помощью этой методики врач получает возможность провести комплексную диагностику мягких и костный тканей колена и системы кровоснабжения этой области. В ходе обследования при помощи специального оборудования — томографа, осуществляется сканирование всех коленных структур с последующей фиксацией полученных результатов на компьютере. После окончания диагностики результаты запечатываются на пленку или диск и передаются пациенту. В отличие от КТ колена или рентгенографии, это исследование не несет лучевую нагрузку, поэтому сделать такую томографию можно как по направлению врача, так и по индивидуальному желанию пациента. Возрастных ограничений у данного сканирования нет. Его проводят как маленьким детям, так и пациентам пожилого возраста, беременным женщинами и больным с онкологическим анамнезом.

Что такое магнитно-резонансная томография коленного сустава
Способ создания снимков при магнитно-резонансной томографии основывается на эффекте ядерного магнитного резонанса атомов водорода в клетках тканей. ЯМР с радиоактивностью никак не связан, поэтому магнитно-резонансное исследование не сопряжено ни с какой лучевой нагрузкой на организм. Просто под воздействием сильного магнитного поля и радиочастотных импульсов протоны в атомах водорода начинают колебаться. Эти движения улавливает компьютер МРТ аппарата и переводит их в изображения тканей и органов. В ходе обследования установка делать множественные изображения в сагиттальной, корональной и аксиальной плоскостях, а затем строит объемные трехмерные черно-белые томограммы коленного сустава и прилегающих областей.

Показания
Врач может назначить магнитно-резонансную томографию в ситуации, если пациент жалуется на хронические боли, снижение подвижности и отечность колена. Помимо диагностики, это обследование позволяет хирургам и травматологам производить подготовку к хирургическим операциям, либо контролировать эффективность медикаментозного лечения.
Когда нужно сделать томографию
Как правило, направление на томографию колена выдает ортопед, травматолог, хирург или ревматолог. Врач направляет пациента на обследования:
- при травме передней крестообразной связки;
- кисте Бейкера (наличие жидкости, скопившейся за коленом);
- при подозрении на инфекционное поражение анатомических структур коленного сустава;
- если симптоматика боли в области колена заставляет предполагать повреждения связок, костей, мышц, сухожилий и хрящей сустава;
- результаты КТ сканирования колена или рентген костей сустава противоречат симптоматике заболевания и пациенту нужно дообследование.
Что видно на томографии колена
В базовый протокол обследования входят следующие структуры:
- суставной хрящ и суставные поверхности надколенника;
- суставные поверхности бедренной и большеберцовой костей;
- связки надколенника;
- сухожилия четырехглавой мышцы бедра;
- суставной хрящ обоих мыщелков большеберцовой кости;
- передняя крестообразная связка;
- задняя крестообразная связка;
- малоберцовая и большеберцовая коллатеральные связки;
- мениски;
- подкожно-жировая клетчатка;
- артерии и вены в зоне колена.
Что покажет МРТ колена
Проведение МРТ при заболеваниях суставов позволит врачу произвести комплексную оценку проблемной области. Проведя сканирование, рентгенолог получает достаточное количество информации для диагностики патологий костной ткани, хрящей, нервных окончаний, кровеносных сосудов, близлежащих мышц, связок, и окружающих сустав мягких тканей. С помощью магнитно-резонансного томографа можно выявить следующие и дифференцировать следующие патологические изменения:
Травматические повреждения:
- разрывы хрящей, менисков, внутрисуставных связок;
- трещины костей;
- повреждения тканевых волокон;
- отек костного мозга;
- закрытые и открытые переломы.
Наличие воспалительных и дегенеративных изменений в хрящевой ткани и костях:
- артриты, бурситы и артрозы;
- хондромаляции суставного хряща;
- субхондральный склероз вдоль суставных поверхностей бедренной и большеберцовой костей;
- деформация межмыщелкового возвышения;
- краевые костные разрастания по краям суставных поверхностей;
- синовиты и тендинозы;
- изменения по типу бедренно-надколенникового конфликта;
Участки с нарушенным кровообращением.
Новообразования злокачественные и доброкачественные;
Изменения плотности костной ткани.
Подготовка
Для МР-исследования колена особая подготовка не требуется. Если нужно сделать МРТ коленного сустава с контрастом, за 2 часа до процедуры врачи рекомендуют отказаться от приема пищи, чтобы избежать рвотного рефлекса.
Если планируется МРТ исследование с контрастом, рентгенологу нужно сообщить о любых аллергиях на препараты.
При проведении исследования у пациентов, страдающих клаустрофобией или психическими расстройствами, может потребоваться прием седативных препаратов.
Если у человека есть боязнь замкнутого пространства, иными словами клаустрофобия, или металлосодержащие или электронные компоненты в организме — это может стать противопоказанием к томографии. Обо всех особенностях своего здоровья или наличии имплантов в теле нужно обязательно сообщить при записи на МРТ. Это поможет врачу сделать правильный выбор в сторону той или иной методики диагностирования. В случае противопоказания альтернативой МРТ станет УЗИ или КТ колена.
Если больной испытывает сильную боль и не может сохранять неподвижность, следует принят перед походом в медицинский центр обезболивающие препараты. Для быстрого купирования боли врачи иногда проводят перед МРТ процедуру блокады сустава. Блокада – это временное медикаментозное “выключение” одного из звеньев механизма развития боли. Осуществляется путем введения медикаментов определенного действия в виде уколов (чаще всего это местные анестетики) в область колена.
В диагностический центр лучше всего взять с собой назначение от врача, а также имеющиеся медицинские документы и данные предварительных исследований.
МРТ коленного сустава с контрастированием
В случаях подозрения на опухоль клинический специалист может назначить проведение МРТ коленного сустава с контрастированием. Контраст делает изображения мягких тканей на снимках более заметными, что облегчает диагностику новообразований и воспалительных процессов. Решение о целесообразности применения контраста обычно принимает лечащий доктор. Если пациент сам принял решение пройти магнитно-резонансную томографию колена в качестве профилактики, начинать свой диагностический путь лучше с базовой МРТ колена без контраста.
Противопоказания
К абсолютным противопоказаниям относятся:
- Установленные кардиоcтимулятор, инсулиновая помпа, если в паспорте импланта не стоит отметки о его совместимости с МРТ;
- Наличие клипс после операций на сосудах;
- Металл в теле: металлические (не титановые) спицы, пластины, скобы, стальные протезы в теле, аппарат Илизарова.
МР-исследование имеют ряд относительных противопоказаний:
- Масса тела более 150 кг;
- Клаустрофобия.
Конструкция закрытых томографов затрудняет обследование людей, страдающих клаустрофобией, или весящих более 150 кг – в этих случаях рекомендуется проводить сканирование на открытых аппаратах.
Если в процессе процедуры предполагается использование контрастного вещества, то список противопоказаний расширяется, и контрастирования не проводится при наличии:
- аллергий на препараты содержащие гадолиния;
- заболеваний почек с нарушением их функции;
- сахарного диабета в стадии декомпенсации.
Как проходит томографии
В диагностическом кабинете пациент ложится на стол томографа. При проведении сканирования требуется непродолжительное время лежать, не двигаясь. Четкость полученных снимков и достоверность результатов во многом зависят от правильности и точности выполнения этих указаний. Обследование длится в среднем 20-30 минут. По окончанию процедуры рентгенолог начинает процедуру расшифровки томограмм. Это занимает 40-60 минут.
По результатам томографии коленного сустава необходимо записаться на консультацию к своему лечащему ортопеду или травматологу, который уже назначает правильную терапию или направляет к более узкому специалисту.
Расшифровка
КТ, МРТ или УЗИ колена — что лучше
Вопрос, что лучше выбрать — МРТ или УЗИ коленного сустава, не имеет однозначного ответа. Диагностические возможности современных УЗИ аппаратов позволяют хорошо визуализировать мягкие ткани (мышцы и сухожилия), окружающие коленный сустав, однако исследование хрящей и костей колена на ультразвуке затруднено. Дело в том, что волна ультразвука не может пройти через кость, поэтому повреждения костных и хрящевых структур при данной диагностике будут видны плохо. Недоступны ультразвуку и глубокие отделы в коленном суставе, например, средние части менисков и крестообразные связки. Но при ультразвуковом обследовании медики могут хорошо оценить состояние кровоснабжения тканей коленной области в динамике, чего не может дать ни МРТ, ни КТ, ни рентген.
УЗИ суставов занимает в среднем 10 минут, и является полостью безболезненным для пациента видом обследования. Привлекательность этого метода в его дешевизне и отсутствие каких-либо противопоказаний. Для врача ультразвуковое исследование сустава — это способ оценить состояние колена в динамике. В ходе исследования диагност может попросить пациента подвигать коленом и посмотреть как выглядит сустав во время движения, и как меняется позиция мышц и костей. Будучи статичными видами обследования, когда обязательным условием успешности сканирования является неподвижность пациента, МРТ и КТ колена не могут дать рентгенологам такой возможности.
МРТ коленного сустав по сравнению с УЗИ будет более информативно по качеству получаемых изображений. Томография позволит оценить как поверхностные ткани, так и глубинные связки и хрящи. Если в ходе УЗИ обследования врач обнаружит опухолевые патологии или аномалии в суставной сумке, пациента оправят на дообследование с помощью МРТ.
Компьютерная томография коленного сустава является приоритетным методом диагностики костных повреждений. КТ коленного сустава лучше, чем МРТ, покажет состояние костей, переломы и костные опухоли. По данным компьютерной томографии врачи могу судить о степени остеопароза и остеонекроза. Поскольку КТ является более быстрой формой сканирования, когда за 2-3 минуты специалист может получить все нужные данные, именно ее используют в случае экстренной диагностики.
| Наименование исследования | Минимальная Цена в СПб | Скидки |
|---|---|---|
| МРТ плечевого сустава |
от 3340 руб. бесплатный прием ортопеда |
Ночью |
| МРТ плечевого сплетения (МРТ шейный отдел позвоночника и плечевого сустава) | от 4600 руб. | Ночью |
| МРТ локтевого сустава |
от 3340 руб. бесплатный прием ортопеда |
Ночью |
| МРТ лучезапястного сустава | от 4000 руб. | Ночью |
| МРТ суставов кисти руки | от 4000 руб. | Ночью |
| МРТ тазобедренных суставов (пара) |
от 3340 руб. бесплатный прием ортопеда |
Ночью |
| МРТ коленного сустава |
от 3340 руб. бесплатный прием ортопеда |
Ночью |
| МРТ голеностопного сустава |
от 3340 руб. бесплатный прием ортопеда |
Ночью |
| МРТ суставов стопы ног | от 3500 руб. | Ночью |
| МРТ височно-челюстных суставов | от 3800 руб. | Ночью |
| МРТ сустава с контрастом | от 6500 руб. | Ночью |
Где лучше сделать томографию колена
При наличии направления КТ суставов можно бесплатно сделать в муниципальной больнице. Для этого лечащий врач поликлиники оформит квоты и поставит пациента на лист ожидания. Период ожидания в среднем составляет месяц. В Санкт-Петербурге услугу томографии предоставляют коммерческие диагностические центры и КТ-кабинеты. На платной основе человек получает возможность пройти обследование без очереди, в любое удобное время, на современном томографе. При выборе частного медицинского центра следует обращать внимание на:
- Характеристики томографа. Огромную роль в успешности томографии играет мощность оборудования. МРТ суставов оптимальнее проводить на аппаратах 1,5 Тесла (если врачом не рекомендовано 3 Тл). Если у пациента есть страх замкнутого пространства, рентгенологи советуют проходить МРТ колена на открытом томографе.
- Квалификация специалиста. Заранее узнайте информацию о враче-рентгенологе: опыт работы, квалификацию. В идеале он должен иметь высшее медицинское образование одного из ведущих образовательных учреждений.
- Консультация специалиста. Если после исследования в медцентре пациент хочет получить не только заключение, но еще и консультацию ортопеда по результатам МРТ, стоит уточнить этот вопрос еще на этапе записи, так как эта услуга не всегда предоставляется бесплатно.
Источники:
- Брюханов A.B., Буевич Е.И. Магнитно-резонансная томография в диагностике ревматоидного артрита // Терапевт. Архив. 2001. — №4. — с. 37-40.
- Блинов H.H., Мазуров А.И. Медицинская рентгенотехника на пороге XXI века // Медицинская техника. 1999. — № 5. — с. 3-6.
- Campbell SE, Sanders TG, Morrison WB. MR imaging of meniscal cysts: incidence, location, and clinical significance. AJR. 2001.
- Laundre BJ, Collins MS, Bond JR, et al. MRI accuracy for tears of the posterior horn of the lateral meniscus in patients with acute anterior cruciate ligament injury and the clinical relevance of missed tears. AJR. 2009.
- Shelbourne KD, Jennings RW, Vahey TN. Magnetic resonance imaging of posterior cruciate ligament injuries: assessment of healing. Am J Knee Surg. 1999.
Дополнительная информация о томографии

Противопоказания к МРТ — ограничения и риски
МРТ считается одним из самых безопасных методов исследования, но и у него есть ряд противопоказаний. Перед проведением магнитно-резонансной томографии следует убедиться в отсутствии ограничений и принять несложные меры предосторожности, и тогда сканирование пройдет успешно и без вреда для здоровья

Где сделать МРТ в Санкт-Петербурге
Назначить сделать МРТ (или магнитно-резонансную томографию) может практически любой врач от невролога и хирурга до репродуктолога и флеболога. Современные томографические аппараты способны проводить сканирование практический любого органа или части тела. Томографическое обследование — это послойное сканирование. В рамках метода томографии исследование можно сделать на МРТ и КТ. Компьютерная томография получает снимки с помощью рентгеновских лучей. Магнитно-резонансная томография визуализирует мягкие и костные ткани с помощью регистрации эффекта колебания атомов водорода в магнитном поле при воздействии на них радиочастотными импульсами.

Можно ли сделать МРТ бесплатно по полису
Отвечая на вопрос, можно ли сделать МРТ бесплатно по ОМС в медицинских центрах СПб, утвердительно скажем — да, но только если у вас есть время и силы ходить по кабинетам. Обязательное медицинское страхование — это возможность всем гражданам России вне зависимости от места рождения и проживания получать лечебную помощь. В перечень диагностических медицинских услуг магнитно-резонансная томография, наряду с компьютерной
Может ли МРТ дать ошибочные результаты?

МРТ (магнитно-резонансная томография) — метод диагностики с высокой точностью. В результате обследования врач получает снимки, на которых видны многочисленные срезы исследуемого органа, направленные в плоскостях. После завершения процедуры на специальном оборудовании, все полученные изображения появляются на компьютере. Может ли МРТ ошибаться в диагнозе? Это зависти от ряда факторов. Все, начиная с подготовки к процедуре и заканчивая заключением врача, имеет прямое отношение к точной постановке диагноза.

Как часто возникают ошибки
Точность результатов МРТ-исследований зависит от томографов: от силы напряжения магнитного поля и мощности градиентов. Чем они будут выше, тем качественнее будет обследование. Старые томографы выдают меньшее количество снимков, они отличаются низким качеством.
Точность МРТ составляет 98%. Ошибки на стадии диагностики составляют 34% от всех первичных диагнозов (то есть каждый третий диагноз – неверный).
Статистика утверждает, что МРТ является точным методом. После сканирования необходимого органа доктор получает полную информацию о состоянии мышечной ткани, сосудов, костей, лимфатических узлов. Аппарат для проведения МРТ не делает никаких выводов о состоянии пациента, не анализирует изображения, не определяет болезнь органа. Томограф – инструмент для трансляции снимков на компьютер врача. После обследования специалист ставит пациенту диагноз.
Причины постановки неверного диагноза
Если пациент неправильно лег в аппарат, могут быть ошибочные снимки. Перед процедурой врач обязан проверить положение человека и правильно выбрать область томографирования. К примеру, смещение подголовника вследствие неверной укладки пациента, дает ошибки в интерпретации томограммы головного мозга. Правильная укладка пациента возможна под контролем трех оптических центраторов, а не только по одному боковому.

Появление артефактов на изображениях – дополнительная проблема. Артефакты – это погрешности, которые допускает доктор в процессе исследования, они способны ухудшить качество снимков. Большая часть артефактов не приводят к ошибкам в чтении результатов. Однако иногда они могут копировать патологические состояния. К подобным артефактам можно отнести:
- артефакты от движения;
- магнитной восприимчивости;
- усечения;
- химического сдвига;
- наложения.
Неправильный выбор методики проведения обследования
Для диагностики серьезных заболеваний, нельзя проводить МРТ без контрастирования. Процедура для диагностирования онкологических заболеваний без контрастирования не сможет указать очаги расположения метастазов, размер и структуру маленькой опухоли. МРТ с контрастированием позволит увидеть мельчайшие метастазы, которые при обычной диагностике не заметны, и поставить более точный диагноз.
Нарушения при подготовке и проведении исследования со стороны пациента
Если планируется МРТ кишечника и органов брюшины, за несколько часов до этого пациент должен отказаться от твердой пищи. Важное условие в момент процедуры – полнейшая неподвижность человека. Ведь самое незначительное движение смазывает изображение, оно уже не будет достоверным. Так как исследование может занимать достаточно долгое время (от 20 до 60 минут), то лучше всего предварительно опустошить кишечник и мочевой пузырь. Маленьким детям нужно выпить седативные лекарства.
Из одежды желательны натуральные ткани. С себя нужно снять посторонние предметы – часы, цепочки. Рентгенолог обязательно узнает о наличии зубных металлических протезов, имплантатов, содержащих металл, кардиостимуляторов, внутриматочных спиралей. Нельзя проходить процедуру при беременности (первый триместр – прямое противопоказание). При наличии татуировок возможен ожог тела. Для пациентов с массой тела более 110 кг диагностика не проводится.
Низкая квалификация специалиста рентгенолога
Значительная часть допущения ошибок возникает на этапе чтения результатов МРТ. Это вопрос компетентности и квалификации врачей радиологов. Чтобы проводить обследование и правильно интерпретировать результаты, важно знать информацию о заболеваниях и диагнозах.
От врача требуются знания:
- Анатомии и патологии. Ведь на срезе можно за патологию принять просто особенность строения органа.
- Правила получения лучевых признаков заболевания. Как процессы в органе влияют на МРТ.
- Симптоматика лучевых заболеваний. По каким признакам на МРТ определяют заболевание.
- Клиническая диагностика.
Бывает так, что пациент прошел исследование на новейшем оборудовании, но врач не сумел правильно и качественно интерпретировать снимки. К частым ошибкам специалиста по чтению МРТ относят:
- Неправильно диагностировать заболевание, перепутав состояния;
- Неверно определить конкретно стадию заболевания;
- Пропустить болезнь, не заметив патологических изменений на срезах;
- Перепутать норму с патологией, диагностировав заболевание, которого нет.

Что делать, если вы сомневаетесь в результате
Пациенты после МРТ-исследования обращаются за консультацией врачей радиологов или других узких специалистов, по чьей направленности проводилась процедура. На данном этапе врач сможет детально вникнуть в проблему, учитывая сведения о пациенте: результаты МРТ-исследования, необходимые анализы, выводы из изучения анамнеза. Только это позволит определить причину патологических изменений.
Сомневающимся пациентам результаты исследований можно отправить на расшифровку другому специалисту. Второе мнение для пациентов необходимо в том случае, если есть сомнения в правильности имеющегося описания или оно вовсе было утеряно. Второе мнение – это своего рода независимая экспертиза от другого врача лучевой терапии.
Подведение итогов
МРТ не может ошибаться в постановке диагноза. Определяет заболевание лечащий врач по снимкам с аппарата. Нужно выбирать специалиста с большим опытом в чтении снимков МРТ. Также неверный процесс процедуры может повлиять на точность диагноза для пациента.
Источник: diagme.ru
Расшифровка МРТ коленного сустава

Магнитно-резонансная томография дает исчерпывающую информацию о состоянии мягких тканей организма. При исследовании колена (одного из самых сложных сочленений) диагностическая процедура качественно дополняет результаты рентгена или КТ. По МР-снимкам оценивают структуру хрящей, связок, мышц, суставных капсул. Сведения о мягкотканных элементах позволяют уточнить диагноз и назначить эффективную терапию. Залогом успешного лечения выступает грамотная расшифровка МРТ коленного сустава.

МР-скан коленного сустава в Т1 режиме (стрелкой указан костный отек)
В структуру сочленения входит множество мелких элементов. Правильно прочитать томограммы сможет специалист в области рентгенологии с внушительным практическим опытом. В спорных ситуациях результаты МРТ предоставляют для чтения нескольким врачам. Человек без медицинского образования и соответствующих навыков не сможет расшифровать снимки. Чтобы понять заключение рентгенолога, требуются глубокие знания. По этой причине трактовку результатов МР-томографии лучше доверить врачу (травматологу или ортопеду).
В основе метода лежит явление ядерно-магнитного резонанса. Это свойство протонов водорода специфическим образом реагировать на индуцируемое аппаратом поле. Заряженные частицы меняют траекторию движения и возвращаются в первоначальное состояние. Томограф улавливает энергетические всплески, компьютерная программа преобразует данные в картинку. Метод специфичен относительно рыхлых структур и биологических жидкостей, поскольку в них есть вода (соответственно, атомы водорода).
При МРТ получают серии монохромных снимков анатомической области в аксиальной, сагиттальной и фронтальной плоскостях. При изучении изображений врач видит контуры различных элементов сочленения. Расшифровка МРТ-снимка коленного сустава подразумевает оценку сканов в сравнении с нормой. МР-томограммы называют срезами, поскольку изображения производят послойно, с шагом 1-2 мм. Врач последовательно изучает анатомическую зону на предмет соответствия всех структур норме. В процессе расшифровки фото обращают внимание на качество визуализации элементов, четкость контуров, присутствие зон измененного МР-сигнала (гипер- или гипоинтенсивного) в различных режимах сканирования (Т1 ВИ, Т2 ВИ, ДВИ, подавление жира).

МР-снимок коленного сустава в режиме Т2, контузия кости
Для повышения качества визуализации используют контрастирование. Введение в организм препарата гадолиния обеспечивает более выраженную реакцию атомов водорода на магнитное поле. В результате увеличивается контрастность снимков, появляется возможность выявить мельчайшие очаги патологических изменений и оценить особенности кровообращения в сочленении.
Норма МРТ коленного сустава
На МР-томограммах сочленения обычно визуализируют:
- суставные поверхности костей;
- надколенник;
- мыщелки;
- мениски;
- ретинакулумы;
- сухожилия;
- связки (надколенника, крестообразные, боковые);
- тело Гоффа;
- мягкие ткани, окружающие сочленение;
- суставная сумка;
- синовиальная жидкость.
Состояние каждого элемента описывают в протоколе исследования. Соответствие анатомической структуры норме может обозначаться как «обычная конфигурация и расположение», «правильная форма», «без особенностей» и пр. Патологические изменения описывают произвольно («неоднородное повышение МР-сигнала», «скопление жидкости», «смещение» и пр.).
Чтобы расшифровать МРТ коленного сустава, нужно в совершенстве владеть знаниями анатомии сочленения и хорошо разбираться в особенностях МР-картины различных заболеваний. Снимки должен читать опытный врач-рентгенолог.
МР-изображение субхондрального перелома латерального мыщелка (зона повреждения указана стрелкой)
Как читать результаты МРТ?
Протокол магнитно-резонансной томографии подытоживают заключением. В этом разделе документа интерпретируют патологические изменения, обнаруженные на срезах. Заключение МРТ коленного сустава может выглядеть так:
«На серии томограмм картина выявлена латеропозиция надколенника, повреждения медиального удерживателя и хондромаляция хряща последнего. Умеренный посттравматический отек тела Гоффа. Экссудативный синовит. Бурсит инфрапателлярной сумки. Умеренный отек мягких тканей в подколенной области».
В заключении МРТ обозначают суть и распространенность патологических процессов. При выдаче результатов рентгенолог может кратко пояснить медицинские термины и порекомендовать пациенту, к какому врачу обратиться.
Расшифровка фото не является диагнозом. Это дополнительная информация для лечащего врача. Диагноз установят на основании результатов МРТ и других исследований, клинической картины и анамнеза.